

Can you smell that?
Can you smell that?
Symptom comparison of radiation poisoning and Covid-19, Part 1

We have observed in previous articles that there is a good case for suspecting radiation plays a part in Covid-19. There is a masquerade surrounding the ‘virus’; its shortlisted supposed genetic components, its source (Wuhan Lab or Wuhan Lab), and the list of two or three ubiquitous symptoms (exploding over the last year into a vast list). We have spent some time splitting the long list into groupings and looking for correlations between the two conditions.
It might help for us to look at the more unusual symptoms first, those that seem unrelated to any cold or flu that we have experienced before.
Nose and Mouth
The loss of smell (anosmia) and taste (ageusia) has been widespread and was highlighted as the third or fourth symptom by UK and international media. Cue objection - we always lose our olfactory senses with flu or a cold. Granted, we do, and things can taste stronger or make us feel slightly yucky. This was different. With flu and colds we generally experience sinus and nasal blockage and excess mucus.
With Covid, taste and smell disappeared with absolutely no sign of mucus or blockage. Instead the onset was frequently accompanied by a sense of extreme thirst and dryness, sometimes nose bleeds, a sensation of burning in nose and mouth, and/or severe headache which seemed to come from the sinus passages across the skull, even though they were not physically blocked. The thirst would seem impossible to quench. The eyes often also felt gritty and dry, with reduced lacrimation (lack of natural tear production). Food would also start to taste odd before the core symptoms set in.
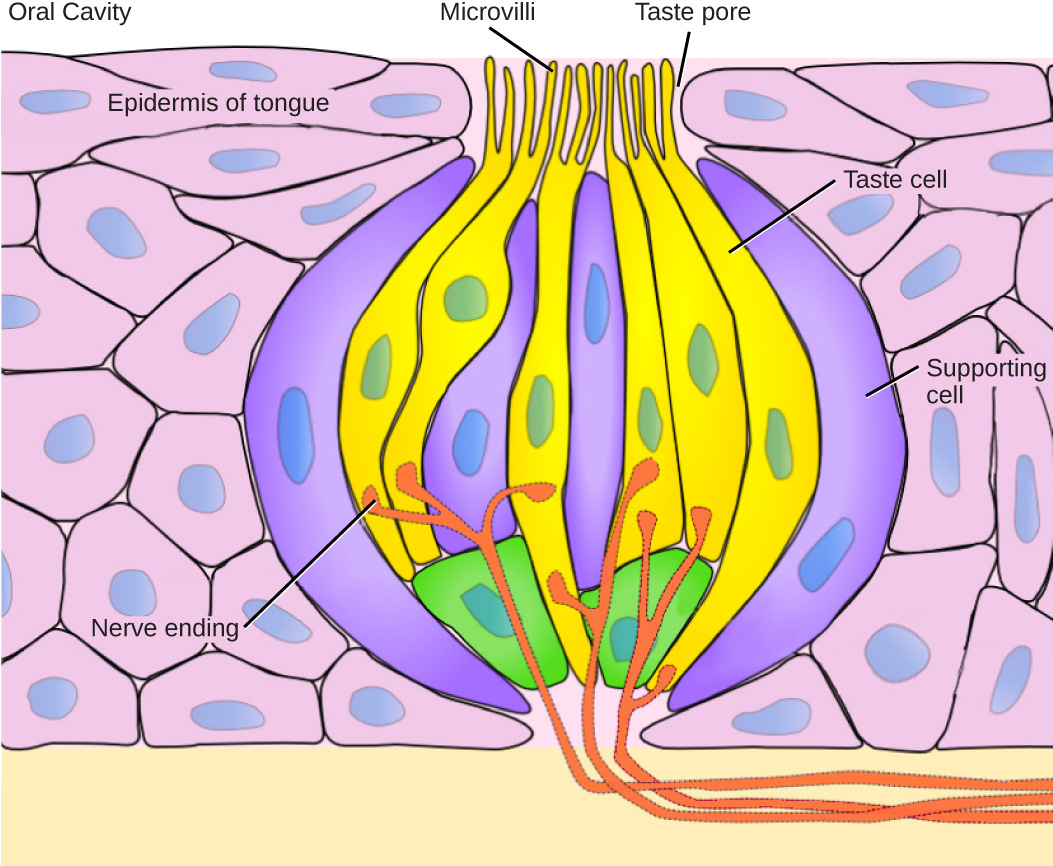
In this article by Harvard, they note that the symptom is not neurological, that it occurs because of damage to the ‘olifactory support cells’ (cells in the nose and mouth that detect taste and smell). Research concludes that this happens because these cells are rich in ACE2 receptors, which are proteins on the surface of the cell that attract Covid-19, as are the kidneys, lungs, blood system and parts of the gut. But, as always, we question that conclusion, as we are seeing effects of Covid throughout the body including in the brain and eyes.
What we propose is that cells closest to the surface of the respiratory tract are the most likely to come in to contact with radiation and therefore suffer the most immediate and obvious damage, where someone experiences acute exposure. The surface of the tongue is relatively tough in comparison to mucus membranes in the side of the mouth and nasal passages but these taste pores with support cells may be more vulnerable from a structural point of view.
This other Harvard article suggests that olfactory senses come back far quicker than they do with other viral illnesses such as flu. However, from our observations, the opposite is true, with many people reporting loss of taste and smell for many weeks and sometimes months with Covid, whereas with flu and cold, it resolves in a week or two.
In this paper about loss of taste (ageusia) it clearly states that ‘Patients with cancer in any head and neck region receiving radiotherapy can present with ageusia as radiation therapy can injure the taste buds, transmitting nerves, and affect the salivary flow by damaging the salivary glands, resulting in gustatory dysfunction’. The damage to the salivary glands may also give us clues as to why the mouth and nasal passages seem to be excessively continuously dry despite attempts at rehydration. This is called Xerostomia or dry mouth and is present in both Covid-19 and in radiation damage to the salivary glands. ‘The prevalence of xerostomia post-radiation is over 90%.’ The condition can also be brought on by certain drugs, particularly ones that have an anticholinergic action, blocking acetylcholine. It stands to reason that radiation and Covid would also compromise acetylcholine action, which may explain why supplementation has produced benefits for some with Covid.
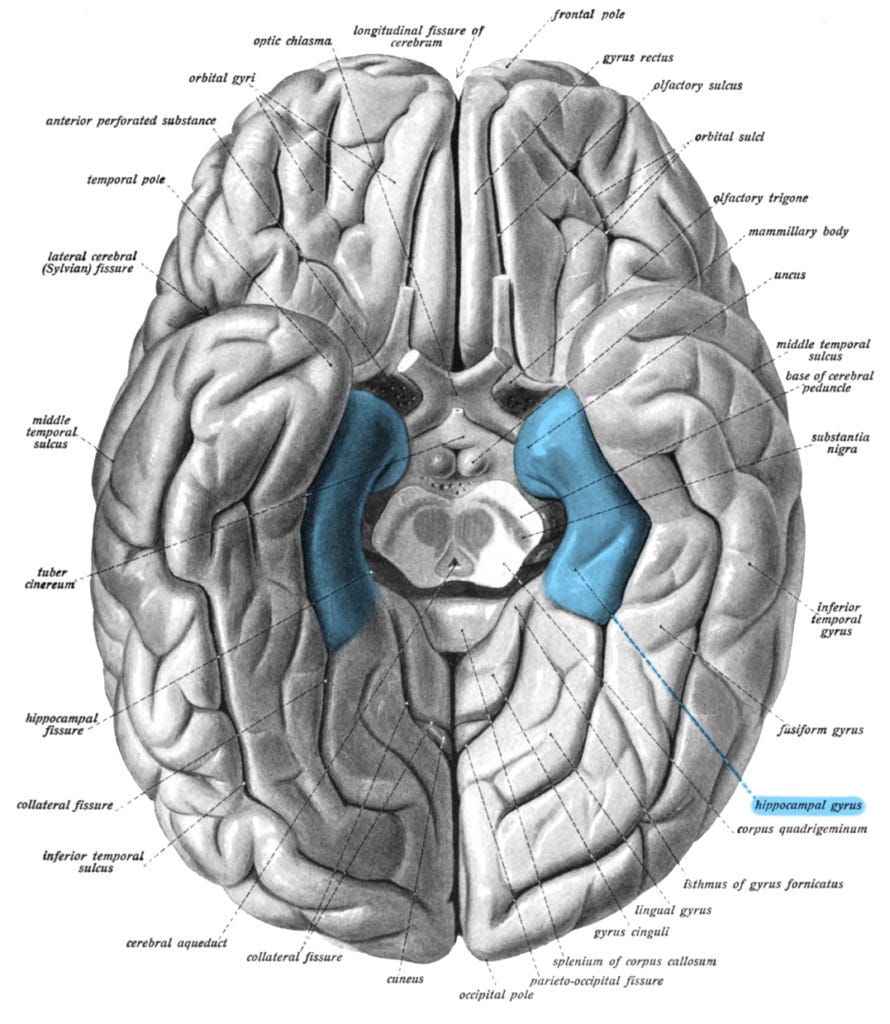
Anosmia (loss of smell) is a well documented side effect of radiotherapy treatment to the neck and head area. Some patients will experience loss for up to 20 months post treatment as the cells struggle to regenerate. The olfactory epithelium (cell lining of the nasal passages) seems to be mildly damaged in the course of radiation, it also appears that the olfactory bulb/orbitofrontal cortex suffers damaged to create the full loss of smell as seen in treatment. This summary of a study conducted on patients with Covid also finds there may be damage to the same region in the brain. Further damage has also been observed ‘in the left parahippocampal gyrus, the left lateral orbitofrontal cortex and the left insula.’ The parahippocampal gyrus is involved in olfactory senses but also in negative emotional reactions and spatial memory. In fact atrophy in this area is also seen as a biomarker of Alzheimer’s disease.
It might seem extremely worrying that the brain is being effected by Covid-19 in a similar way to radiotherapy patients, but the good news is that clearly, as smell and taste return, there is regeneration in these areas of the brain and of all the cells involved in sensing, transmitting and interpreting smell and taste signals. Only 2 patients out of 51 in this French study were still without smell and taste after one year.
The Eyes
Staying with the head, I also want to look at the functional optical issues, as these seem to be significant in Covid patients. Some are also connected with neural symptoms including stroke and migraine which we will look at in another article. There have been frequent reports of dry eye and an array of infections including chemosis and pink eye in Covid-19. These eye infections and loss of lubrication are also found in radiation exposure.
The symptoms of most interest are optical opacities (clouding within the eyeball and other retinopathies (symptoms to do with the retina). In this paper ‘Ocular complications after radiotherapy; an observational study’, dry eye syndrome, conjunctival, cornea, iris, retina and optic nerves can all exhibit dysfunction after irradiation. In August 2020 a summary of ocular dysfunction in Covid-19 included ‘corneal neuropathies, optic neuritis, uveitis, retinitis and an exacerbation of dry eye’ and episcleritis. Whilst they use different terminology these symptom groups are the same.
Some more specific findings in this paper, included hyperreflective lesions in the retina, cotton wool spots and micro hemorrhages within the eyeball in Covid-19 patients. The cotton wool spots and micro hemorrhages are also found in a detailed paper on ‘Radiation Retinopathy’. ‘It was first described in 1933 by Stallard and appears clinically as microaneurysms, telangiectases, neovascularization, vitreous hemorrhage, hard exudates, cotton wool spots and macular edema.’ Microaneurysms are another description for micro hemorrhages.

From the same paper, retinal detachment from radiation exposure is common. The retina is the layer of blood vessel rich tissue on the inner surface of the eyeball and leads to the optic nerve at the back of the eye. Rhegmatogenous detachment, or a detachment of this layer from the inner surface of the eyeball due to a rupture or break, is present in both Covid-19 and radiotherapy patients. A characteristic tear is visible in this image below, and can lead to blindness if not treated.

Cotton Wool Spots are cloud like lesions on the retina. They are also associated with diabetes and HIV and can result in ischemia (lack of blood flow) to parts of the eye, due to their structure blocking the arteriols (blood vessels) in the retina. This feature may well be a result of scarring caused by the micro hemorrhages as seen in both conditions.
Having looked at a few viruses in our searches on symptom sets, we also see a number of these complex optical symptoms appearing in Ebola. Even more interesting is that Ebola has been talked about concurrently with Covid-19 as the next big incoming disease. We will be writing about Ebola and Marburg at a later point.
To date our research has shown no notable differences in array of symptoms for loss of smell and taste or optical pathologies, which leads us to believe that they may well arise from the same cause. If we pair these findings with the PCR DNA analysis of biomarkers for both conditions, we can see that the similarities are starting to pile up.
Next we will be looking at the pulmonary (lung) and cardio (heart/blood) systems features found across both conditions, which promises to be even more interesting.
This is breathtaking.
Thanks to you and your team, great work and analysis. It’s reassuring in our thinking.